The Resurgence of Diphtheria
Borderline
01 Jan 2018
Prevent where you can, cure where you can't
From the Executive Director
Prevent where you can, cure where you can't
Spring has come after winter and warms the earth. While I personally like the transition periods between seasons, they are also conducive to spread of epidemics. We know well how vaccination can help reduce outbreaks; we have it at home, seasonally, with the flu. Yet, lack of access to vaccination, insufficient vaccination coverage, can instead lead to a resurgence of preventable diseases and result in outbreaks.
This issue’s Cover Story features Diphtheria, a bacterial infection which has been eradicated from most countries over the past thirty years. Diphtheria is a preventable disease – for those who are vaccinated against it – and a potentially deadly one for those who are not and who get infected.
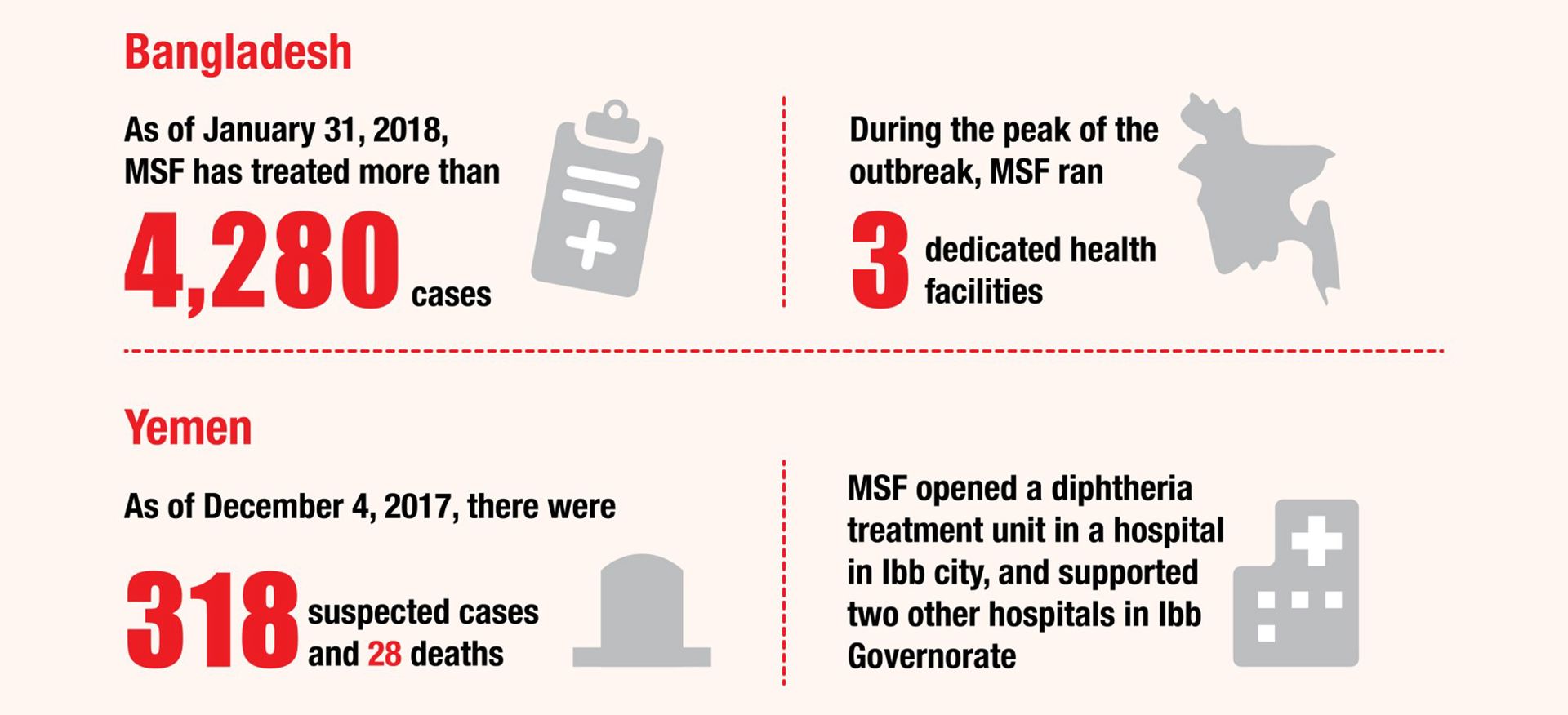
Since August 2017, about 700,000 Rohingya have fled to Bangladesh following targeted violence against them in Myanmar in the last half year. The overcrowded refugee camps and poor water and sanitation conditions there have become breeding grounds for the disease, among a population group who had little access to vaccination in Myanmar. MSF teams identified the first suspected case of diphtheria three months after the Rohingya crisis unfolded – an outbreak had started: This vulnerable population, which had gone through so much trauma, was now being hit by a disease that could have been completely preventable. MSF teams have since then been treating patients and supporting vaccination campaigns.
In another part of the world, armed conflicts in Yemen started in March 2015, dragging the whole country into extreme violence and insecurity, and crushing the health system. When medical facilities can barely operate, people will not be able to get the medical care they require, including basic, essential vaccinations. Following cholera and acute watery diarrhea outbreaks, a suspected diphtheria outbreak took hold in Yemen late last year. Here again, MSF field workers have helped treat patients and implement vaccination campaigns.
Coverage in vaccination campaigns is essential. In many instances, in some of the remote or volatile areas on our humanitarian front lines, even population data or maps can be lacking, outdated or inaccurate. To support our medical field workers, MSF has co-founded the “Missing Maps Project” and organized a number of collective mapping activities, “Mapathons”, gathering volunteers to locate buildings, pathways and water sources based on satellite pictures. Accurate, updated maps help remarkably in the planning and implementation of many of our frontline activities, in the preparedness for future emergencies. This Mapathon endeavor is another feature in this edition of Borderline I strongly recommend.
Preparing for emergencies is an essential part of our work; Mapathon is one of the means to support our preparedness. Vaccination, on another hand, is a powerful prevention measure and we all know well the saying “prevention is better than cure”. But the outrage of preventable epidemics, when, as in Yemen and Bangladesh, patients need emergency treatment, still demand action. This is also our crucial task to bring rapid assistance to the people in need.

Diphtheria: A Disease of the Past Poses a New Threat
Cover Story
Diphtheria: A Disease of the Past Poses a New Threat
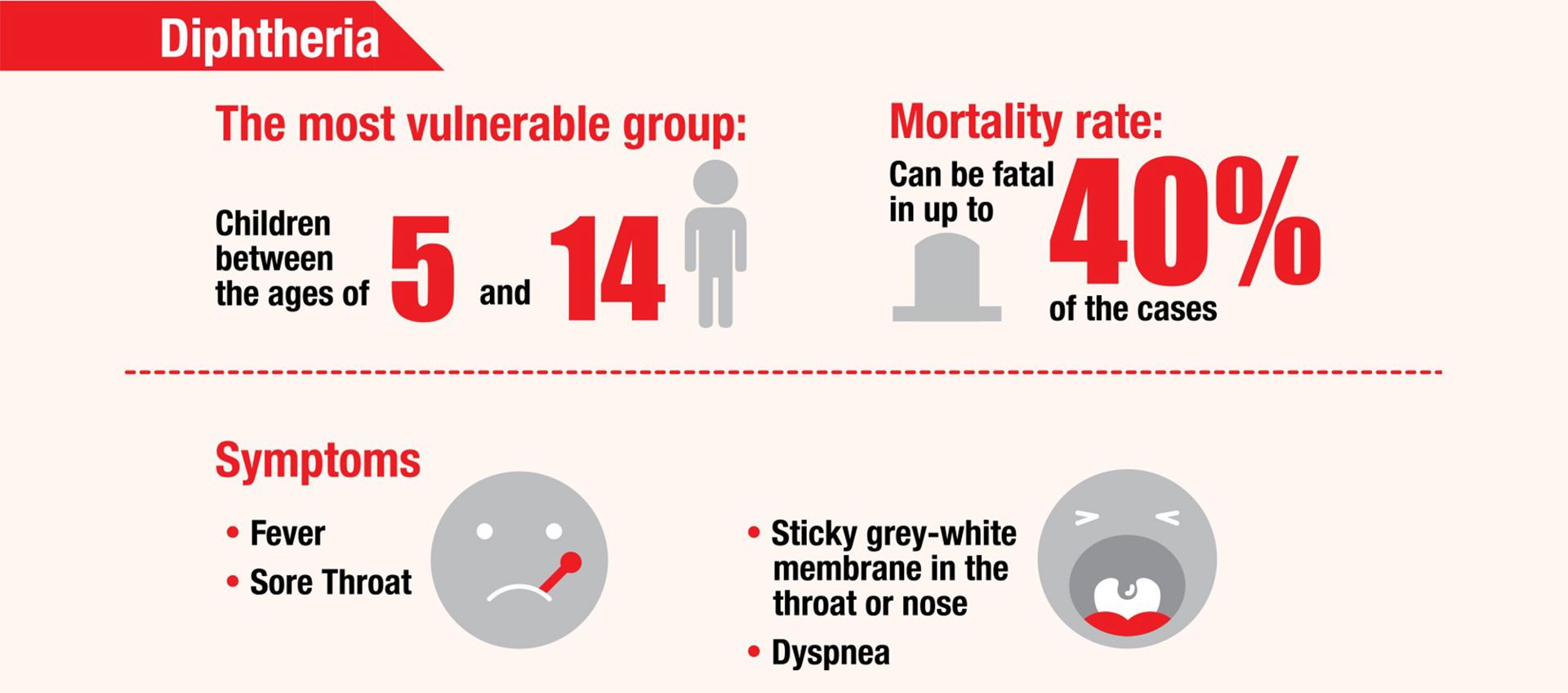
Diphtheria, a contagious and potentially fatal bacterial infection, has been eradicated from most countries after systematic childhood vaccination campaigns over the past thirty years. Yet, humanitarian crises like population displacement and war have caused this neglected and forgotten disease to rage again.
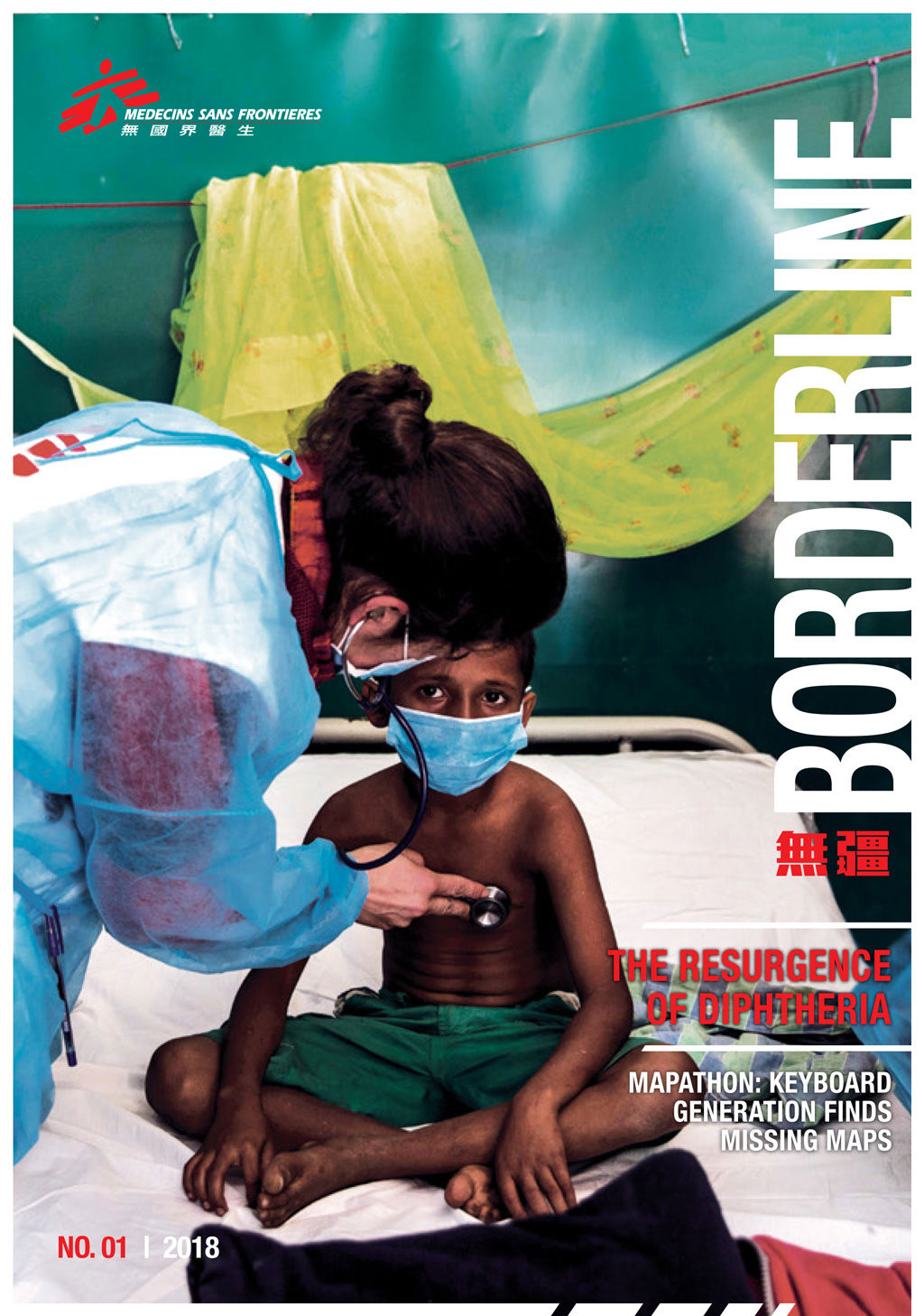
Since late August 2017, nearly 700,000 Rohingya have sought refuge in Bangladesh following increased violence in Myanmar. The population of the border town of Cox's Bazar has grown exponentially within half a year. The refugees are living in over-crowded, precarious makeshift settlements, with shelters squeezed up against each other. Sometimes families with up to 10 people live in one very small space. This provides ideal conditions for disease outbreaks.
In early November , MSF teams there identified the first suspected case of diphtheria. Crystal VanLeeuwen, MSF emergency medical coordinator for Bangladesh was very surprised when she received the news. “‘Diphtheria?’ I asked the doctor calling me, ‘Are you sure?’ When working in a refugee setting you always have your eyes open for infectious, vaccine-preventable diseases such as tetanus, measles and polio, but diphtheria was not something that was on my radar,” said VanLeeuwen.

Diphtheria is a contagious bacterial infection that often causes the buildup of sticky grey-white membrane in the throat or nose. The infection is known to cause airway obstruction and damage to the heart and nervous system.
The disease is vaccine-preventable. For instance in Hong Kong, the government began the “Hong Kong Childhood Immunisation Programme” in 1960s, providing a range of free vaccinations for children up to the age of twelve That includes diphtheria, tetanus and acellular Pertussis & Inactivated Poliovirus Vaccine (DTaP-IPV Vaccine). The successful implementation of the programme relies on the comparatively well -developed healthcare system in the city.
The resurgence of diphtheria in Bangladesh highlights how vulnerable Rohingya refugees are. The majority of them are not vaccinated against any diseases, as they had very limited access to routine healthcare, including vaccinations, back in Myanmar. Coupled with the very cramped living conditions and poor hygiene in the refugee camps, as soon as the first case appeared, the disease, which is spread by respiratory droplets, turned into an outbreak.
A few months before diphtheria raged in Bangladesh, a suspected diphtheria outbreak took hold in Yemen. The last diphtheria case there was recorded in 1992, and the last outbreak in 1982.
“The ongoing war and the blockade on supplies including medicines and vaccines are sending Yemen’s health system decades back in time. The healthcare infrastructure is in tatters. The blockade on fuel has meant that patients cannot afford to travel to the very few health centres still operating across the country,” said Marc Poncin, MSF’s emergency coordinator in Ibb. “This is crucial, because if people infected are unable to access treatment regularly, diphtheria can spread in the body and be fatal in up to 40 per cent of the cases. What is more, the country was barely recovering from a massive cholera outbreak, with over one million suspected cases,”
The Rohingya and the Yemeni population have been through so much trauma – war, violence, forcible displacement – and they were just hit by a disease that is completely preventable with only basic access to healthcare and a routine vaccination that was invented over 90 years ago.

The Jamtoli makeshift settlements are packed with overcrowded populations and poor sanitation condition which provide a favorable condition for the spread of diseases. © Anna Surinyach

“We had to learn around the clock how to treat diphtheria”
With the last major outbreak happening decades ago, most MSF staff had only seen diphtheria in textbooks. Teams in Bangladesh confronted a lot of challenges in treating the disease.
“When diphtheria broke out in December 2017, the MSF team was completely overwhelmed. Given the urgency of the situation, we decided to put the construction of a brand new hospital on hold and focus on setting up a diphtheria treatment centre in the hospital grounds. Initially housed in a series of tents, the treatment centre was later moved into several of the completed wards,” said Carla Pla, MSF Medical Team Leader.
“In those early weeks, it was difficult to manage. Patients were arriving all at once, sometimes in minibuses, and at the same time our staff were not very experienced. We had only seen this in textbooks, but never experienced anything like this before. The last outbreak of diphtheria happened decades ago. We had to learn around the clock how to treat patients for diphtheria.”
“Once the diagnosis is confirmed, the most delicate part of the treatment is administering diphtheria antitoxin (DAT). The medication is given intravenously and can produce adverse reactions leading to complications, and even death, if not well managed. One-to-one patient-clinician care is necessary, particularly at the start, because you have to detect side effects quickly to be able to address them.”
DAT can effectively reduce the fatality rate of diphtheria. But there is a global shortage of DAT, with less than 5,000 vials available currently. It becomes an ethical and equity question when there is not enough life-saving medication to treat all patients, and MSF medics are often left to make extremely difficult decisions.
Other challenges are to ensure that patients are isolated to prevent the disease from spreading, and identify everyone with whom the patients have been in contact to provide vaccinations and prophylaxis
Apart from providing treatment, it is equally important to vaccinate the population to halt the transmission. MSF has supported the Bangladeshi Ministry of Health to carry out a diphtheria vaccination campaign. This campaign poses more logistical and technical challenges than the previous ones for cholera and measles, as it requires a course of three vaccines administered one month apart.

Behind the Conflict in Yemen
Photo Feature
Behind the Conflict in Yemen
A full-scale war has been raging in Yemen since March 2015 at an immense cost to the people there. The rising cost of living has made it extremely hard for families to meet basic needs. An estimated 14.8 million people – 55% of Yemen’s population – can’t get basic healthcare. More than half of the health facilities are no longer operational because of damage, lacking staff and medicines. In addition, soaring fuel prices make any movement to the remaining facilities unaffordable for most patients who often seek treatment at the last minute. The non-payment of Ministry of Health staff salaries for a whole year is another aggravating factor of the collapse of health system. Apart from the medical needs directly caused by conflict, there were over one million suspected cholera cases between April 2017 to February 2018, followed by a suspected outbreak of diphtheria. In order to respond to the mounting needs, MSF works in or provides support to 33 hospitals and health centers in 12 governorates.





Mapathon: Keyboard Generation Participating in Medical Humanitarian Action
MSF Knowledge
Mapathon: Keyboard Generation Participating in Medical Humanitarian Action
Despite the rapid development of information technology like satellite photography and Google Earth, many resource-poor countries are still blank spaces on the map. Inspired by Wikipedia, the “OpenStreetMap” platform offers the opportunity for people to participate in making accurate, up-to-update maps, and contribute meaningfully to medical humanitarian work in corners of the world where map information is incomplete.
In the aftermath of the Haiti earthquake in 2010, the Typhoon Haiyan in the Philippines in 2013, and the Nepal earthquake in 2015, the keyboard generation completed mapping the disaster areas very rapidly, and their maps became reliable tools for relief work. In 2014, MSF co-founded the “Missing Maps Project”, which prioritizes mapping vulnerable areas prone to disasters and epidemics. Equipped with more accurate maps ahead of the emergency, humanitarian workers can better follow the impact of natural disasters and epidemic outbreaks, as well as the movements of displaced populations to save more lives.
MSF has organized a number of collective mapping activities, "Mapathons". Volunteers come together to help locate buildings, roads, pathways and water sources based on satellite pictures.
How does cloud mapping help MSF's work?
Taking measles vaccination as an example, in a campaign, 95% of the target population must be vaccinated to successfully stop the spread of the disease. However, if the number of people needing injections is unknown, it is difficult to prepare enough vaccines, refrigeration equipment, related transportation and manpower plans. Having a map with detailed information is then essential.
In April 2016, there was an outbreak of measles in Idjwi, the Democratic Republic of Congo, but the last census was done in 2010. Idjwi is very rural without paved roads or easy access, hampering the launch of a vaccination campaign. MSF gathered volunteers who happened to be taking part in Mapathons held in the UK and Belgium to helpcomplete maps of the area.. Just a week after the outbreak, mapping was completed and handed over to MSF's frontline field teams. 94.8% of the target population received injections, which was an excellent result.
"People are very keen to take part because the outputs are so important, and the whole process offers a fantastic middle ground of support between donating to MSF and volunteering as part of [the organization's] field operations," said Duncan Bain, the UK Mapathon organizer.

In the two Mapathons held in Singapore and Hong Kong, more than 250 participants mapped nearly 9,000 buildings and more than 300 kilometres of roads for Niger State in Nigeria. Accurate maps assist emergency teams in epidemiological data analysis, disease surveillance and logistical planning.
Mapathon participants do not need special skills, and are not norlimited by space or time. They can just log onto their cloud accounts for mapping while they are free, and contribute to medical humanitarian assistance on the front line.


Facing life and death in the early morning in Haiti
Frontline Sharing
Facing life and death in the early morning in Haiti
A Chinese popular proverb says “a day’s plan starts with early morning.” My working day in Haiti starts even before dawn.
One day at four in the morning, we received a man with multiple gunshot wounds in the emergency room at the MSF's Tabarre trauma centre in Port-Au-Prince. Wounds were found on his right chest and right inner elbow. Another bullet entered his right inner thigh and went through the scrotum. The patient was conscious when he was admitted. His blood pressure was normal but his respiratory and heart rates were raised. With multiple examinations including X-ray and ultrasound, we ruled out the possibility of abdominal trauma. We gave him some fluids, and sent him to the operating theatre right away. There we repaired his wounds, and placed a gauze pad in the abdominal cavity to create pressure to stop the bleeding.
The patient later told us that he was injured at 11am the day before. The incident occurred at the city center of Port-au-Prince, which is only a thirty-minute drive away from the trauma centre. Why did it take him so long in seeking treatment?
In fact, shootings happen frequently in Port-au-Prince, and the locals often carry a gun with them when they go out. Gangs are a commonly sight. Our trauma centre is located in the city centre and is easy to reach. But the delay might be because he couldn’t call the ambulance for fear of being arrested by the police during daytime. Or he simply couldn't find a car to take him here. Whatever the reasons, MSF provides medical care to people in need. As long as they abide by our “No Weapons” policy, they are regarded as our patients who should receive treatment. This patient was fortunate, as most of his important internal organs and intestine were not injured, otherwise he could have lost his life.
On another early morning, a patient in her 40s was sent to us. Her right leg had an open spiral fracture of the tibia while the same bone in her left leg was nearly exposed. She did not say a word. The elderly mother who brought her here told us that her daughter SS had mental health problems. She didn't know how the accident had happened to SS at midnight. Fortunately, SS' key blood vessels and nerves were not affected. Other major organs and systems also functioned normally. After surgery, she was transferred first to the recovery room and then to the in-patient ward.
How did SS get hurt? From the wounds on her tibia, SS might have fallen from a higher point or a slope. She might have suffered from a traffic accident. In Haiti, there are few traffic lights. Almost none of the local drivers respect traffic rules. Motorbike accidents are common.
Sadly, SS might encounter similar accidents again because she is a bit more at risk in an already risky environment. Imagine the pressure on her mother, having to care for her daughter and deal with the financial burden at the same time.
For myself, Chinese people place emphasis on right timing, proper location and favorable human resources to complete a mission, which can be applied to saving lives too. I will do my best, which is all I can do.
Jennifer Tong is an orthopaedic surgeon from Hong Kong. After her first field assignment with MSF in Kunduz, Afghanistan in June 2015, she worked in another MSF mission in Haiti from January to April 2018.
Dr. Jennifer Tong, an MSF orthopaedic surgeon very often starts her work before dawn in Port-Au-Prince, Haiti.

The MSF's trauma center is located in the city center of the city, which can be easily accessible for people in need.


Your Decision Can Make A Lasting Impact to Transform Lives
MSF Hong Kong
Your Decision Can Make A Lasting Impact to Transform Lives
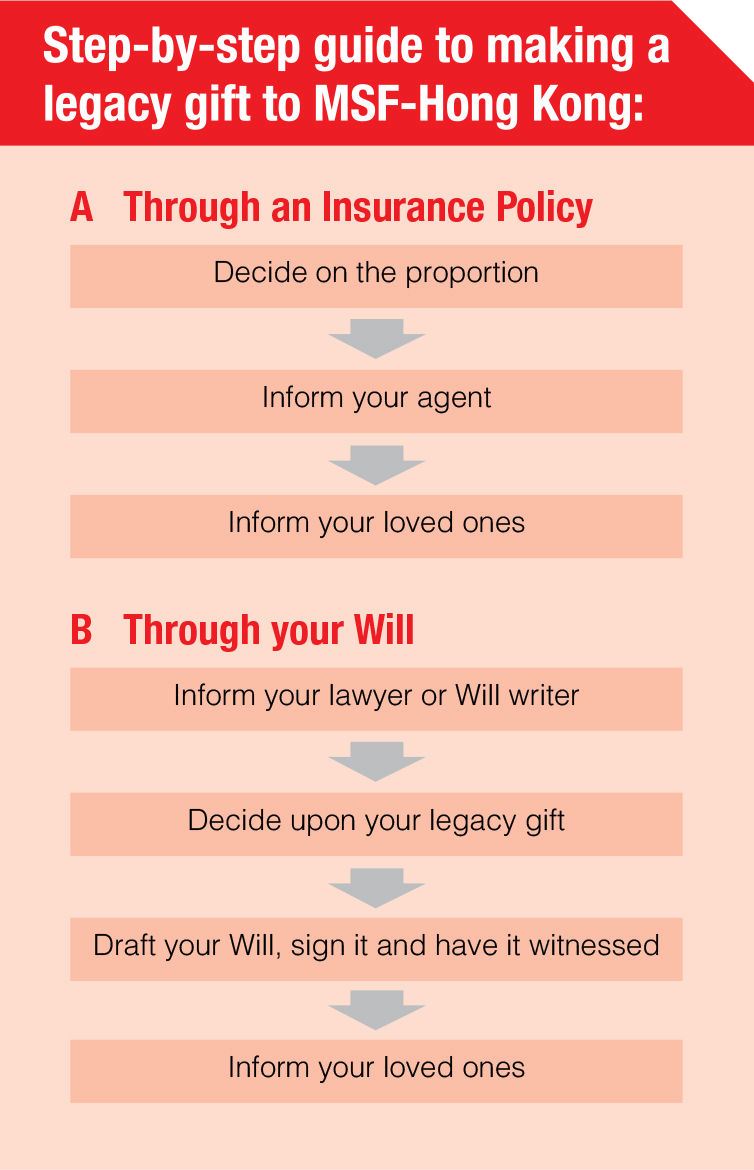
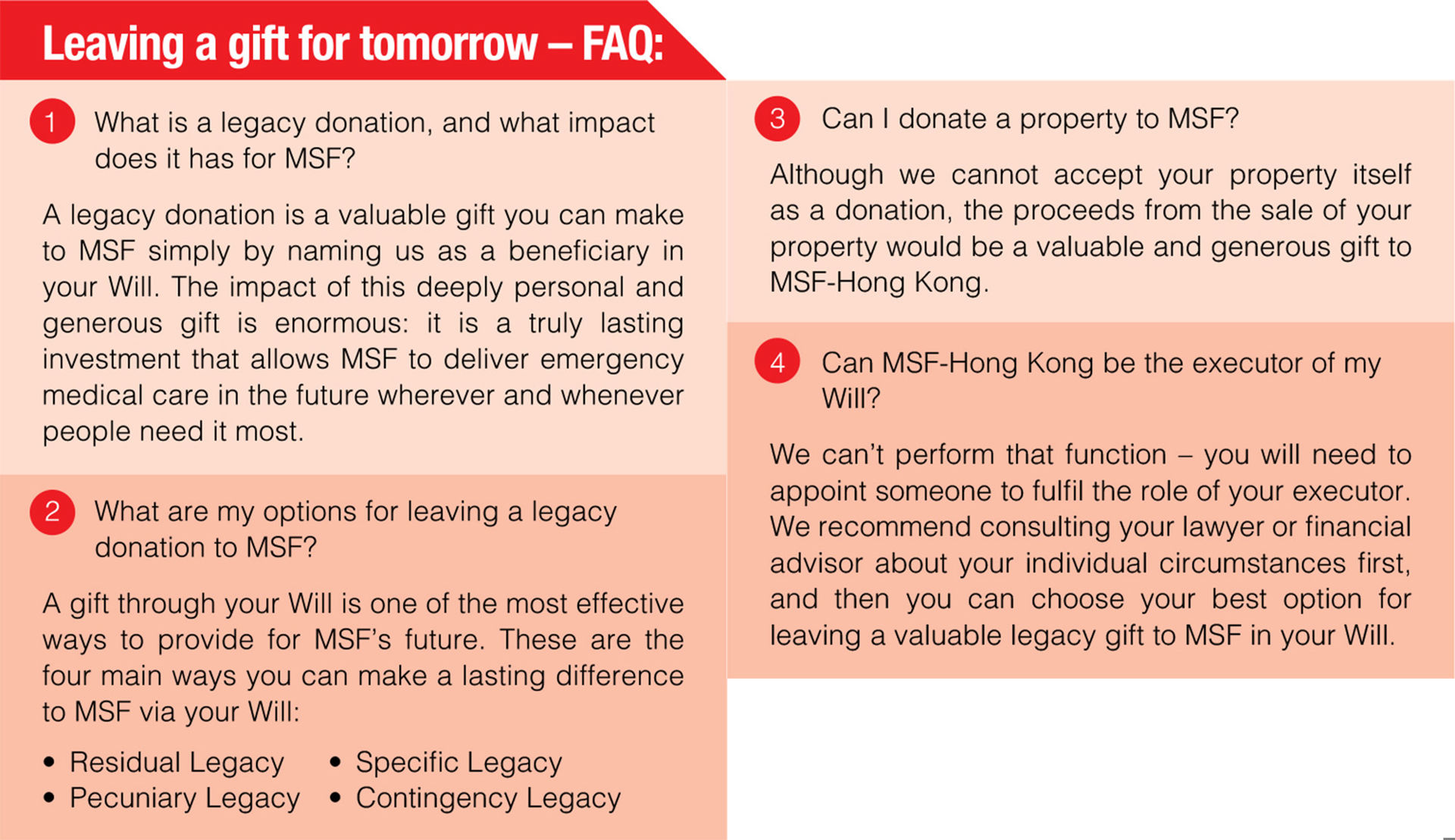
All of us experience illness, either ourselves or through our family. Fortunately, few of us would ever experience being forced from our homes by violence, conflict or disaster, or suffering without any access to healthcare. MSF’s teams are in the field helping people in crisis with many supporters’ long-run generosity. Someone who truly believes in our work can ensure their compassion has an even bigger impact for years to come, making changes in the world, by leaving a legacy donation as a gift to MSF in their Will.
A legacy donation will help transform the lives of vulnerable people on a daily basis and provide huge support to communities in hard-to-reach rural areas. The generous bequest will also sustain our financial independence to deliver medical humanitarian assistance where the needs are greatest.
What our Legacy Donor says
There may be different motivations for our legacy donors to support us. Dr. John Lawrence from the US thinks that philanthropy is a way of practicing what one preaches. “I’ve seen firsthand how our donors’ contributions go a long way in helping people around the world get medical care. By leaving a gift to Médecins Sans Frontières (MSF) in my will, I know I am creating a legacy that will save lives.”
Dr. Lawrence is currently a paediatric surgeon at Maimonides Medical Center in Brooklyn, New York. Owing in part to a longstanding interest in global health, Dr Lawrence has completed eight humanitarian missions with MSF since 2009. He has served MSF as a surgeon in the Central African Republic, Ivory Coast, Haiti, Syria, and the Democratic Republic of Congo, and was appointed president of the board of directors of MSF-USA in 2016.