Yemen: "A frightening and fatal condition I’d never seen before"
Feb 03, 2017
In our project hospital, the growing need for neonatal and maternal care was clear, as these are the vulnerable groups affected by Yemen’s ongoing war. Unfortunately, we saw an increasing number of sick newborns in our ER who suffered complications relating to poor antenatal care, unhygienic delivery practices and difficult births at home. Poverty, low level of education amongst mothers and the distance from health care facilities only aggravate the problem.
A case I remember vividly is an 8-day-old baby boy who was delivered at home in a village. His mother brought him to ER because he gradually stopped feeding for a few days, and that morning he developed some ‘strange movements’. In front of me was a dehydrated 2.7kg baby: his neck was curved backwards, his limbs were stiff and straight, and his body repeatedly spasmed. Although I’d never seen a case like this before, I immediately recognized this frightening and fatal condition – neonatal tetanus.
Neonatal tetanus occurs only in newborns who have not acquired immunity from a vaccinated mother, particularly when a non-sterile instrument was used to cut the umbilical cord. It hardly exists in developed countries or places like Hong Kong, because it is easily preventable with immunization programs, comprehensive antenatal care and safe delivery practices.
We quickly gave medications (to neutralize the tetanus toxin), an IV drip, antibiotics, and sedatives to control the spasms. His condition slightly improved. However, the spasms continued at a reduced frequency. These spasms in tetanus are easily triggered by surrounding light or sound.
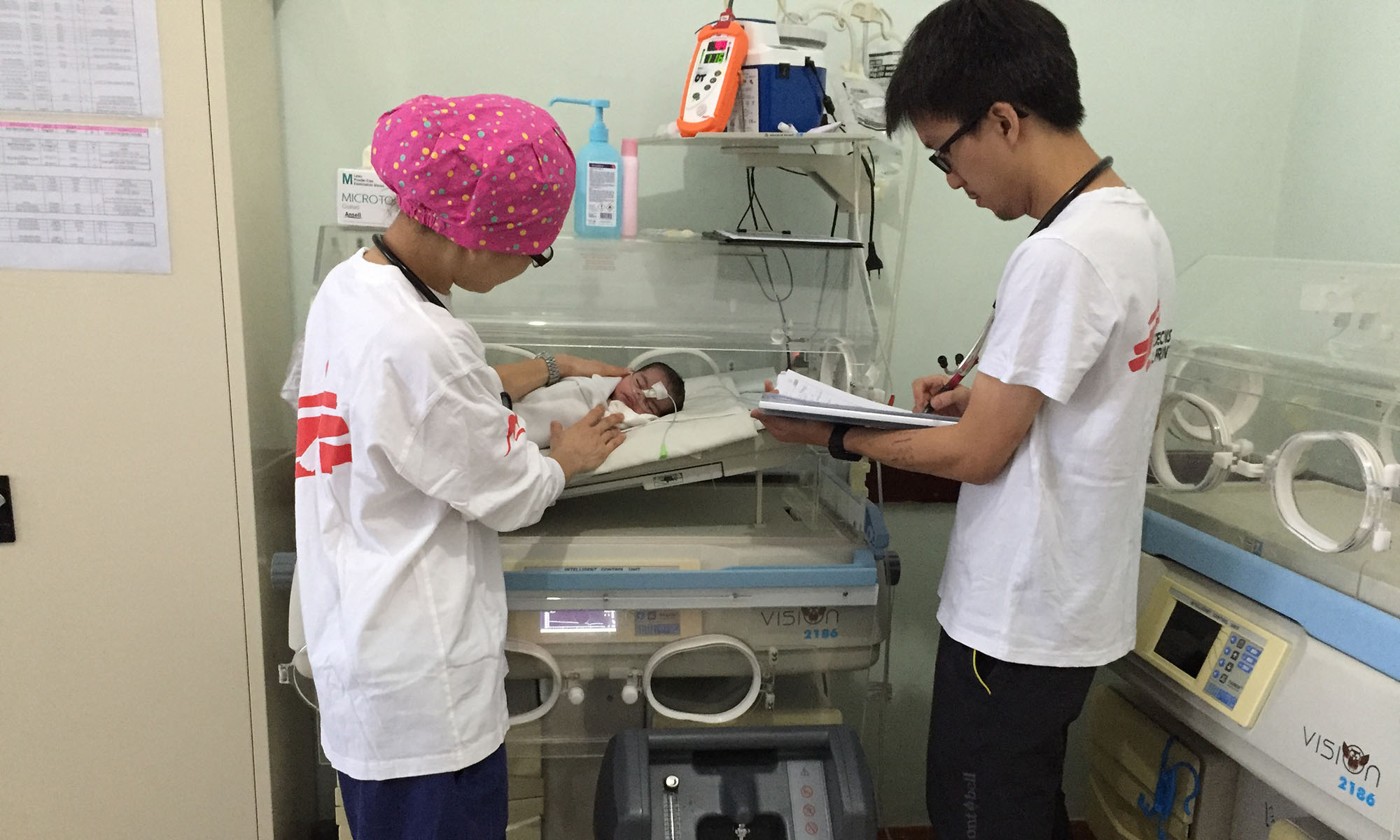
In the next 24 hours, I repeatedly went to the high dependency unit to check his condition. He was inside an incubator almost fully covered by dark cloth. His spasms continued, even to the point where he struggled to breathe. I gradually increased the dosage and frequency of the sedatives. Every spasm was painful for him - it was truly a depressing and unforgettable sight. In the end, I decided to transfer him to an MSF paediatric unit in Taiz, where hopefully a better nursing environment and the paediatrician’s input could increase the chance of his survival. However, the ambulance journey to Taiz could take up to 45 minutes depending on traffic. It was a risk I decided to take. Fortunately, I received confirmation that evening about his safe arrival.
Fortunately, with medications, basic monitoring, proper feeding and parent education, many sick newborns and children were treated and discharged home. Although the mothers and female caretakers’ faces were covered by veils, their expressions of gratitude and happiness shone through. I felt a trust and bonding with them that transcends culture, language and gender. Witnessing their babies’ transition from very ill patients in the ER to thriving babies on discharge was undoubtedly my biggest satisfaction. I hope they will always remember ‘the Chinese doctor’, as they would call me, as someone who went to see their babies at 10 a.m. every morning.
ER doctor Jimmy Leung from Hong Kong worked in the hospital supported by MSF in Ibb governorate, Yemen from August to November 2016 for his first mission with MSF.
Related Articles
Mar 08, 2022

在無國界醫生,有不少出色的女性領導者。無論是在辦事處、後勤支援,抑或前線救援等不同崗位,都不難發現她們的身影。她們在組織內以行動展現女性的力量,確保我們的項目更全面和多元,照顧弱勢群體的醫療需要。她們的貢獻,讓我們得以持續改善組織的政策和工作,並賦權予更多女性,從員工、到我們服務的社區的婦女和女孩。
Dec 18, 2020

陳詩瓏醫生(Shannon)於2016年在南蘇丹首次參與無國界醫生的救援任務,2019年12 月,她到也門穆哈前線醫院參與第二次救援任務,負責醫院的外科部門和培訓當地人員。人民要在穆哈地區獲得醫療服務是一件極為困難的事。有一次,一群無辜的孩子被地雷誤炸,傷亡慘重,讓她感受尤深。 在穆哈,對許多因衝突而流離失所的也門人來說,僅僅走到街上也有可能危及生命。事故涉及9名在街上玩耍的孩子,年齡介乎9至13歲,其中一人踩中地雷,導致再多兩枚地雷相繼爆炸。孩子們未及逃跑,地雷已爆開。...

Leave a Comment