Setting up an Operating Room from scratch




Mar 24, 2017
The recent civil war in South Sudan has been heating up and our surgical team at Bor has received a request for assistance from another MSF project located at Old Fangak.
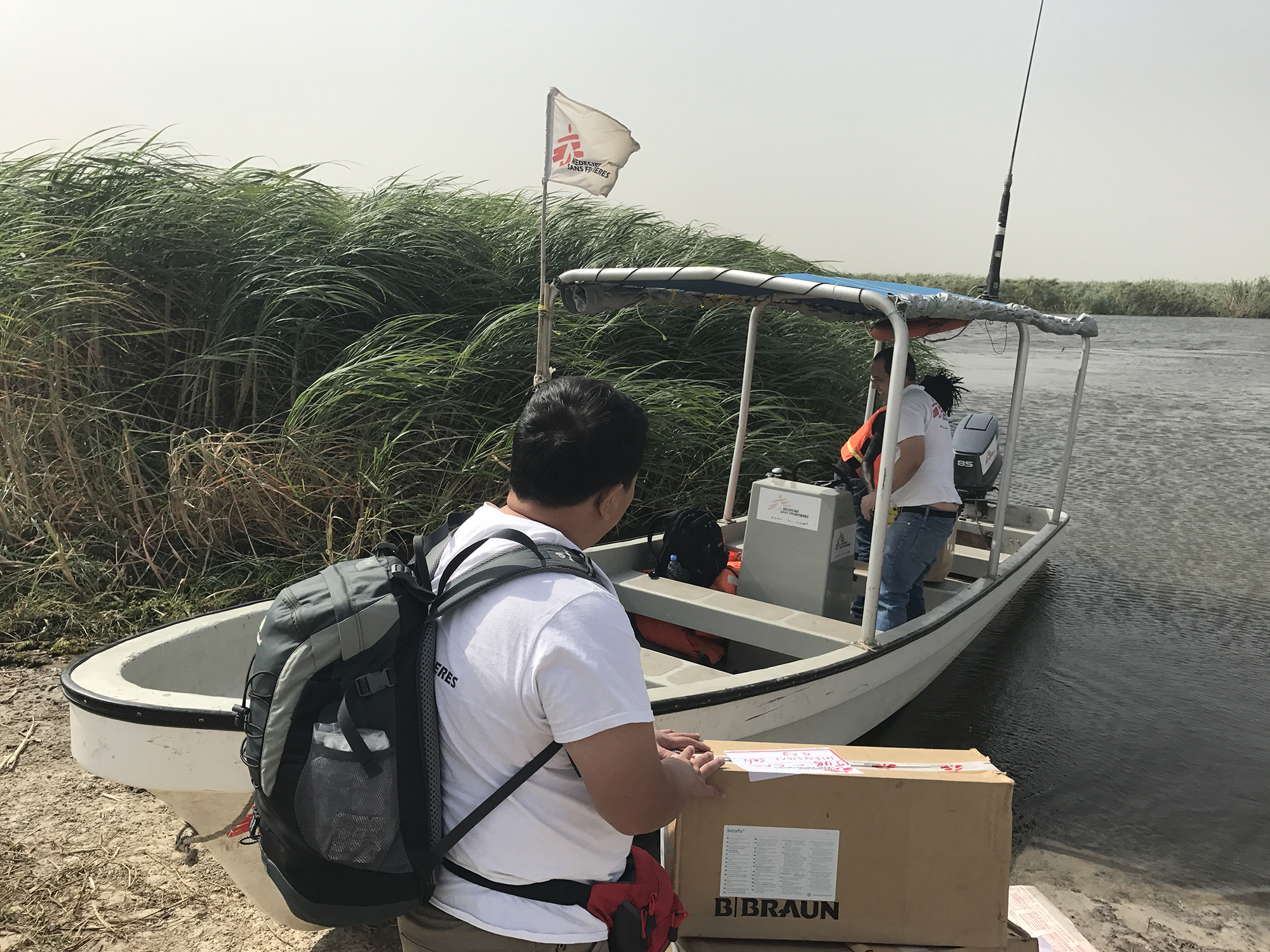
Old Fangak Médecins Sans Frontières hospital is located in the northern part of South Sudan, at the tributary of the Nile River, a high-risk area for tribal conflict. Speedboat is the only way to travel from the front line of the fighting to the hospital.
In the last two weeks, due to active fighting in the area, the Old Fangak hospital has been receiving large numbers of injured. The hospital is small and primarily deals with internal medicine and infectious diseases, and lacks surgical facilities. Considering the deterioration of the situation, the team in the hospital has asked our surgical team to help, hoping to help establish a surgical service to meet current needs.
Our team, consisting of three members: a surgeon (myself), an anaesthetist and an operating room nurse, agreed with no hesitation.
The team's idea is to convert the treatment room, which was originally used for wound dressing, into an operating room. We ordered some basic surgical instruments and supplies from headquarters to be delivered to Old Fangak on the same day we arrived.
We took the MSF flight and arrived at the Old Fangak MSF hospital in about two hours. We immediately started converting the treatment room. We had to set up everything from scratch, including the operating table, operating theatre lights, surgical instruments, surgical gloves, gauze, drugs, and even the trash bin. In addition, we also needed to manage the surgical instrument sterilisation, the waste disposal, operating room cleaning, and the logistic issue. After working really hard for half a day, the “operating room” was finally set up!
Although it was just a simple operating room with no air conditioning, no perfect infection control system, and no advanced surgical instruments, for emergency life- saving purposes, it was the best we could do and perhaps it would be adequate. Though I have practiced for more than a decade and completed countless surgeries, I have never set up an operating room.It was absolutely unprecedented for me! The three of us could not help but be really proud of this!
Just as we thought we could take a break, a 10 year old girl was admitted to the Emergency Room. She had been suffering from stomach pain for two days, with fever and vomiting. After examination, I diagnosed it as peritonitis which needed immediate emergency surgery.
Fortunately, the "operating room" has just been set up, thus we could manage her immediately.
This girl suffered from typhoid fever with small intestine perforation and the entire abdominal cavity was contaminated. I repaired the perforation in her intestine, cleaned the abdominal cavity and the surgery was completed within an hour. Before the surgery, we were worried if the operating room could function well, and we were much relieved after the surgery.
The moment we had completed the first surgery, we were told that there had been vigorous fighting around the area, and that there were more than a dozen wounded patients coming via speedboat along the River Nile.
We started our preparations at once.
Every time when we deal with a large number of wounded patients, an emergency response Mass Casualty Plan (MCP) will be activated. Everyone is assigned a specific role: security guard, crowd control, triage, first aid resuscitation, surgical care, and even psychological support to the attendants. The whole end-to-end arrangement is very important, because the large number of the injured, in addition to their attendants, can make things very chaotic.
When the patients arrived at the hospital, they were triaged based on the severity of their injuries. Those who were in an immediate life-threatening condition, which required resuscitation and surgical treatment, were classified as red; those who were relatively stable and whose treatment could be slightly delayed, yellow; those who were in mild and not immediate life-threatening condition, green; those who were dead or in a dying state were classified as black. So we were determining the treatment priority based on how critical their conditions were. Yet, the situation may change at any time, so we needed to repeat the assessment and, if there was any deterioration, the treatment priority would be changed. In addition, crowd control is extremely important. Usually every wounded patient is accompanied by several attendants. If everyone rushed into the Emergency Room at the same time, the situation would be extremely chaotic. So prior staff training and thorough preparation is very important.
Two boats arrived at 11pm with a total of 16 patients with gunshot wounds. After the initial assessment, one was red, nine yellow, and six green. For the red wounded, with gunshot wounds in his abdomen and wrist, and signs of peritonitis, emergency surgery was immediately arranged.
Upon opening up the abdominal cavity, I found both of his large and small intestines were penetrated by bullets.It was necessary to conduct resection of the large and small intestine, and to fashion a temporary stoma, in other words an artificial anus, for defecation. After nearly three hours, the surgery finally finished. Looking at the watch I realized it was already 4am in the morning. There were nine other patients to follow. One surgery after another, we eventually completed all the cases at 8pm the next day. Our surgical team was absolutely exhausted.
Although it was so busy in the first two days, all three of us were very glad that all the patients were well treated and recovering. Now was the time to rest, and God knows when the next mass casualty will arrive again.
Truly we wish that the war will end as soon as possible!
Related Articles
Mar 08, 2022

在無國界醫生,有不少出色的女性領導者。無論是在辦事處、後勤支援,抑或前線救援等不同崗位,都不難發現她們的身影。她們在組織內以行動展現女性的力量,確保我們的項目更全面和多元,照顧弱勢群體的醫療需要。她們的貢獻,讓我們得以持續改善組織的政策和工作,並賦權予更多女性,從員工、到我們服務的社區的婦女和女孩。
Dec 18, 2020

陳詩瓏醫生(Shannon)於2016年在南蘇丹首次參與無國界醫生的救援任務,2019年12 月,她到也門穆哈前線醫院參與第二次救援任務,負責醫院的外科部門和培訓當地人員。人民要在穆哈地區獲得醫療服務是一件極為困難的事。有一次,一群無辜的孩子被地雷誤炸,傷亡慘重,讓她感受尤深。 在穆哈,對許多因衝突而流離失所的也門人來說,僅僅走到街上也有可能危及生命。事故涉及9名在街上玩耍的孩子,年齡介乎9至13歲,其中一人踩中地雷,導致再多兩枚地雷相繼爆炸。孩子們未及逃跑,地雷已爆開。...

Leave a Comment